Vendor managed inventory is often described as simply “letting the supplier handle ordering.” That framing misses most of what actually matters. In healthcare supply chains, where stockouts can delay procedures and expired products carry serious compliance consequences, VMI is a governance model as much as a logistics one. Getting it right requires deliberate decisions about data sharing, threshold ownership, contract structure, and traceability. This article explains how VMI works operationally, where healthcare organizations commonly go wrong, and what a well-designed implementation actually looks like in practice.
Table of Contents
- Key Takeaways
- How vendor managed inventory works in practice
- Data accuracy and visibility in healthcare VMI
- Benefits, risks, and contract design in healthcare VMI
- Practical steps for implementing VMI in healthcare
- What most VMI implementations get wrong
- How Labgistics supports healthcare VMI
- FAQ
Key Takeaways
| Point | Details |
|---|---|
| Governance determines outcomes | Decide explicitly who owns min/max thresholds before launch to avoid replenishment errors at the wrong locations. |
| Data accuracy is non-negotiable | Regular cycle counts and real-time consumption visibility are prerequisites for supplier-driven replenishment to function correctly. |
| Contract terms shape incentives | Pay-on-consumption models align supplier behavior with your interests far better than pay-on-delivery arrangements. |
| Traceability protects compliance | RFID and UDI tracking reduce overstocking, support FEFO rotation, and compress recall investigation timelines in regulated environments. |
| Expect an iterative tuning period | Initial replenishment parameters rarely match steady-state performance; plan for structured adjustment over the first few cycles. |
How vendor managed inventory works in practice
Vendor managed inventory shifts replenishment decisions to the supplier, using shared inventory and consumption data to trigger restocking within agreed boundaries. The buyer no longer issues purchase orders on a reactive basis. Instead, the supplier monitors stock levels continuously and initiates replenishment when on-hand quantities fall below agreed minimums.
The operational flow follows a recognizable sequence:
- Data sharing: The buyer shares real-time or periodic inventory and consumption data with the supplier through an electronic portal or EDI connection.
- Threshold monitoring: The supplier monitors stock against pre-agreed minimum and maximum quantities at the item or storage location level.
- Replenishment trigger: When on-hand inventory drops below the minimum, the supplier creates a replenishment request or purchase requisition.
- Order conversion and fulfillment: The request converts to a purchase order, the supplier ships product, and the system records the transaction for invoicing.
- Invoice and payment: Depending on the contract model, invoicing occurs either on delivery or upon consumption of the stock.
In Oracle’s VMI model, suppliers manage min/max thresholds directly and replenish when on-hand falls below the minimum, with purchase requests converting automatically to fulfillment orders. This automated sequence reduces the manual coordination burden that typically drives up order lead times.
A critical but often overlooked design question is who owns the min/max thresholds. Thresholds can be governed by either the enterprise or the supplier, and the configuration can apply at the item level or at the sub-inventory level. Getting this wrong means replenishment logic may be technically correct but applied to the wrong storage location, producing stockouts in one ward while another holds excess.
| Governance model | Threshold ownership | Best suited for |
|---|---|---|
| Enterprise-controlled | Buying organization sets min/max | High-regulation items, critical care products |
| Supplier-controlled | Vendor uploads and manages thresholds | High-volume commodity consumables |
| Hybrid | Shared responsibility with approval workflows | Medical devices with variable demand |
Pro Tip: Before signing any VMI agreement, document threshold ownership explicitly in the contract. Define whether the enterprise or the supplier controls each parameter, and specify the approval process for any threshold changes.
Data accuracy and visibility in healthcare VMI
Shifting replenishment responsibility to suppliers only works if the data they receive is accurate. Buyers must invest in real-time consumption visibility to enable replenishment triggers that reflect actual usage, not stale figures from batch uploads. In a hospital ward environment, where consumption can spike unpredictably, lagged data translates directly into stockouts or overstock.
Healthcare VMI adds complexity that general distribution models do not face. Consider the following requirements that apply specifically to regulated healthcare inventory:
- FEFO and FIFO rotation: Products must be issued by First Expiry First Out or First In First Out principles to minimize waste and prevent expired product from reaching patients. Automated stock management systems need to enforce these rules at the point of dispensing, not just at the point of receipt.
- Cycle counts and reconciliation: Inventory accuracy via regular cycle counts reduces stockouts and waste in regulated healthcare environments. Counts should be scheduled based on product criticality, not on administrative convenience.
- Serialized and UDI tracking: For medical devices, Unique Device Identification tracking creates an unbroken chain of custody from manufacturer to point of use. This is a regulatory requirement in many Southeast Asian markets, not a optional enhancement.
- Exception handling protocols: When a count discrepancy exceeds an agreed tolerance, there must be a defined process for investigation and correction before the next replenishment cycle runs.
The practical impact of RFID-based traceability is well documented. Real-time product visibility via RFID supports traceability and reliability for healthcare supply chains, reducing over-purchasing and compressing product recall investigation timelines to approximately 24 hours. For organizations managing high-value implants or temperature-sensitive biologics, that capability is operationally significant.
Practitioners should define cycle count frequencies and exception thresholds before the system goes live. VMI replaces buyer-driven orders with supplier-driven triggers, meaning data errors flow directly into ordering decisions without the manual review step that previously caught discrepancies.

Pro Tip: Segment your inventory by criticality and assign cycle count frequencies accordingly. High-value, expiry-sensitive items warrant weekly counts; lower-risk consumables may only require monthly reconciliation.
For healthcare organizations exploring how traceability technologies integrate with 3PL warehouse operations in Singapore, RFID-enabled fulfillment centers represent the infrastructure foundation that makes data-accurate VMI feasible at scale.
Benefits, risks, and contract design in healthcare VMI
VMI delivers measurable financial benefits when implemented correctly. Reduced days sales in inventory, improved cash flow, and lower carrying costs are the most frequently cited gains. Memorial Hermann’s health system, for example, improved fill rates and reduced stockouts using data-driven supply chain decision-making. These are not theoretical outcomes. They reflect what happens when replenishment is driven by actual consumption data rather than purchasing guesswork.
That said, the financial structure of a VMI contract determines whether supplier behavior reinforces or undermines those gains.
- Pay-on-delivery risk: When suppliers are paid on delivery rather than on consumption, they have a financial incentive to ship to the maximum threshold at every replenishment cycle. Consignment models and pay-on-consumption arrangements better align incentives, with the supplier benefiting only when product is actually used.
- Consignment stock considerations: Consignment arrangements keep product ownership with the supplier until consumption is confirmed. This improves the buyer’s working capital position but may carry a small price premium. Understanding how consignment medical equipment arrangements work in practice helps procurement teams negotiate terms that reflect actual risk transfer.
- Initial parameter drift: Initial replenishment parameters often require adjustment after two to three cycles. First-run min/max settings are estimates. Actual demand data from the first few weeks routinely reveals that some items are set too high and others too low.
- Stockout and overstock monitoring: Both failure modes are costly in healthcare. Overstock ties up working capital and creates expiry risk; stockout risks patient care. Performance monitoring must track both, not just service levels.
“Incentive misalignment in contracts is a common hidden failure risk in VMI. Pay-on-consumption models better align interests than pay-on-delivery.” — VMI Implementation Guide, User Solutions
Healthcare procurement teams reviewing supplier contracts will also find value in surgical supplies sourcing practices that address vendor managed supply chain considerations specific to medical settings.
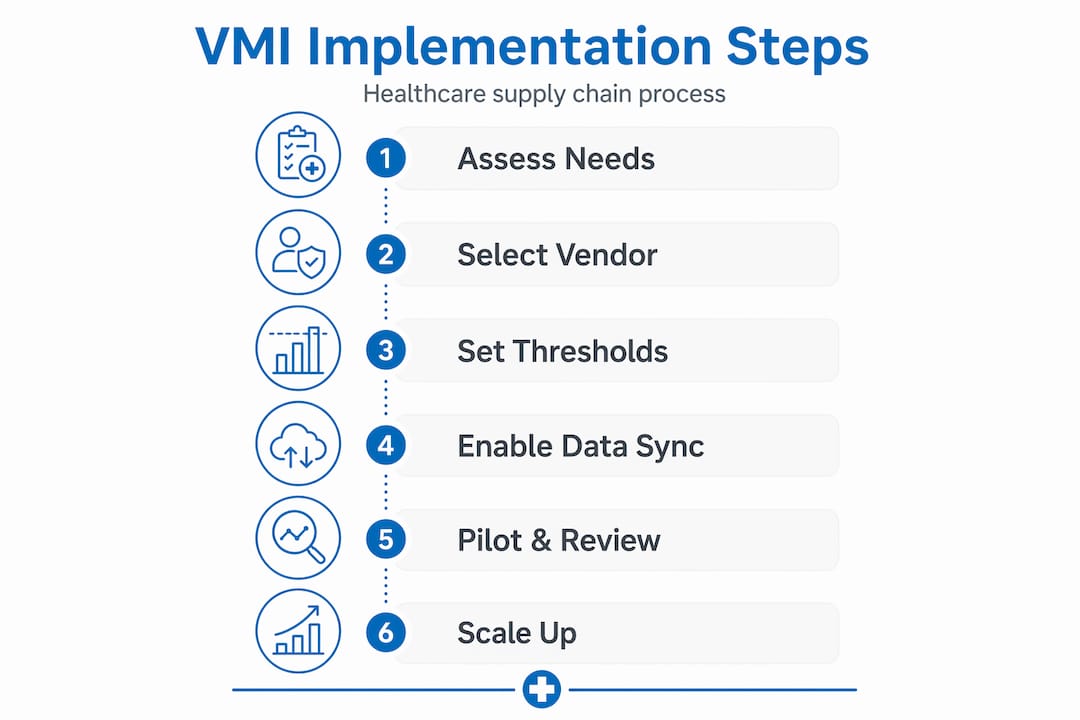
Practical steps for implementing VMI in healthcare
Successful implementation requires more than selecting a software platform. The following steps reflect the governance and operational requirements specific to healthcare supply chains.
-
Define threshold ownership and governance. Before any data flows, document who sets min/max quantities for each item category, how changes are approved, and which organization retains final authority over replenishment decisions. Governance arrangements must clarify roles and decision rights beyond simple data exchange.
-
Invest in data integration and supplier portals. Real-time consumption data must reach suppliers through a reliable, structured channel. EDI, API-based portals, or shared cloud platforms are all viable depending on supplier capability. Batch file transfers create latency that undermines the replenishment model.
-
Design contract terms that align incentives. Include performance KPIs covering fill rate, on-time delivery, expiry management, and documentation accuracy. Specify payment terms that favor consumption-based triggers. Define consequences for threshold changes made without approval.
-
Build traceability and compliance into the workflow. For pharmaceuticals and medical devices, traceability is not optional. Serial number capture, UDI recording, cold chain documentation, and FEFO rotation rules should be embedded in the receiving and dispensing SOPs from day one.
-
Plan for iterative tuning. Treat the first 90 days as a calibration period. Schedule structured reviews at 30, 60, and 90 days to assess replenishment accuracy, adjust thresholds, and address exception patterns before they become systemic.
-
Train staff and establish continuous improvement processes. Warehouse and clinical staff interacting with VMI stock need to understand the replenishment logic, how to flag discrepancies, and why accurate transaction recording matters. A shared dashboard visible to both buyer and supplier supports accountability on both sides.
For teams building out inventory management best practices in healthcare logistics, these six steps provide a practical framework that addresses the governance, technology, and compliance dimensions together.
Pro Tip: Run a parallel operation for the first replenishment cycle. Keep your existing ordering process active alongside VMI so you can compare outputs and catch configuration errors before they affect patient care.
What most VMI implementations get wrong
From my experience working with healthcare supply chain teams across Southeast Asia, the single most common failure point in VMI adoption is treating it as a technology deployment rather than a governance redesign. Organizations spend months selecting vendor inventory systems and configuring portals, then launch without a clear answer to the question of who owns the thresholds. Within weeks, replenishment is technically functioning but restocking the wrong sub-inventory locations.
I’ve also seen teams underestimate how much upfront data quality work is required. VMI amplifies whatever errors already exist in your inventory records. A 95% inventory accuracy rate sounds acceptable until you realize that a 5% error rate across hundreds of SKUs in a hospital setting means dozens of items with incorrect stock signals driving automated replenishment decisions.
What genuinely works, in my experience, is pairing governance clarity with iterative threshold tuning. The organizations that perform best treat the first three months as a structured learning process, not a steady-state operation. They review replenishment outcomes weekly, adjust parameters, and document every exception. By month four, their min/max settings actually reflect demand patterns at their specific sites.
The traceability piece is also consistently underinvested. Teams that integrate RFID or serialized UDI tracking from the start report far fewer expiry write-offs and a dramatically shorter recall response window. Given that regulatory scrutiny on medical device traceability is intensifying across Southeast Asia in 2026, that investment pays for itself in compliance terms alone.
— Labgistics
How Labgistics supports healthcare VMI
Labgistics brings over 20 years of specialized experience in healthcare logistics across Southeast Asia, making it a capable partner for organizations implementing or optimizing vendor managed inventory programs. Its fully accredited distribution centers in Singapore are equipped for compliant pharma logistics, including cold chain management, serialized product tracking, and FEFO-compliant storage and dispensing.
For supply chain professionals navigating medical device regulatory compliance requirements, Labgistics provides regulatory services that align inventory processes with HSA standards and regional market requirements. Its end-to-end capabilities cover the documentation, validation, and traceability infrastructure that VMI contracts in regulated healthcare environments demand.
Whether you are building a VMI program from the ground up or addressing gaps in an existing supplier inventory control arrangement, Labgistics offers the operational expertise and infrastructure to support your goals. Contact the Labgistics team to discuss how its healthcare supply chain advantages can be applied to your specific inventory management challenges.
FAQ
What is vendor managed inventory in healthcare?
Vendor managed inventory is a supply model where the supplier monitors inventory levels and initiates replenishment based on agreed minimum and maximum thresholds, using shared consumption data from the buyer.
How do min/max thresholds work in a VMI system?
Min/max thresholds define the lower and upper stock levels that trigger replenishment. Either the buying organization or the supplier can own these parameters, and threshold configuration scope applies at the item or sub-inventory level depending on the system setup.
What are the main risks of VMI for healthcare organizations?
The primary risks include supplier over-shipment under pay-on-delivery contracts, data inaccuracies driving incorrect replenishment, and misaligned threshold governance leading to stockouts or overstock at specific locations.
How does RFID support VMI in regulated healthcare settings?
RFID enables real-time inventory visibility that supports traceability, FEFO rotation enforcement, and rapid recall response. RFID-based traceability has been shown to compress product recall investigation timelines to approximately 24 hours.
How long does it take for VMI to reach stable performance?
Most implementations require two to three replenishment cycles before min/max settings reflect actual demand accurately. Planning a structured 90-day tuning period with regular threshold reviews is standard practice for healthcare VMI programs.