The medical device regulatory environment has never moved faster. In 2026, manufacturers and regulatory affairs teams face compounding pressures: FDA’s Quality Management System Regulation (QMSR) took effect on February 2, 2026, incorporating ISO 13485 into US law for the first time; EU MDR Notified Body backlogs continue straining certification timelines; and global reliance programs are reshaping how multi-market strategies get structured. Understanding these shifts is not optional. For regulatory affairs professionals operating across multiple jurisdictions, clarity on these frameworks directly determines market access timelines and audit outcomes.
Table of Contents
- Key Takeaways
- Medical device regulatory frameworks: a global overview
- FDA QMSR: what changed in 2026 and why it matters
- EU MDR certification challenges and practical strategies
- Global reliance frameworks and multi-market strategy
- Best practices for lifecycle compliance in 2026
- My perspective on navigating regulatory complexity in 2026
- How Labgistics supports your regulatory compliance journey
- FAQ
Key Takeaways
| Point | Details |
|---|---|
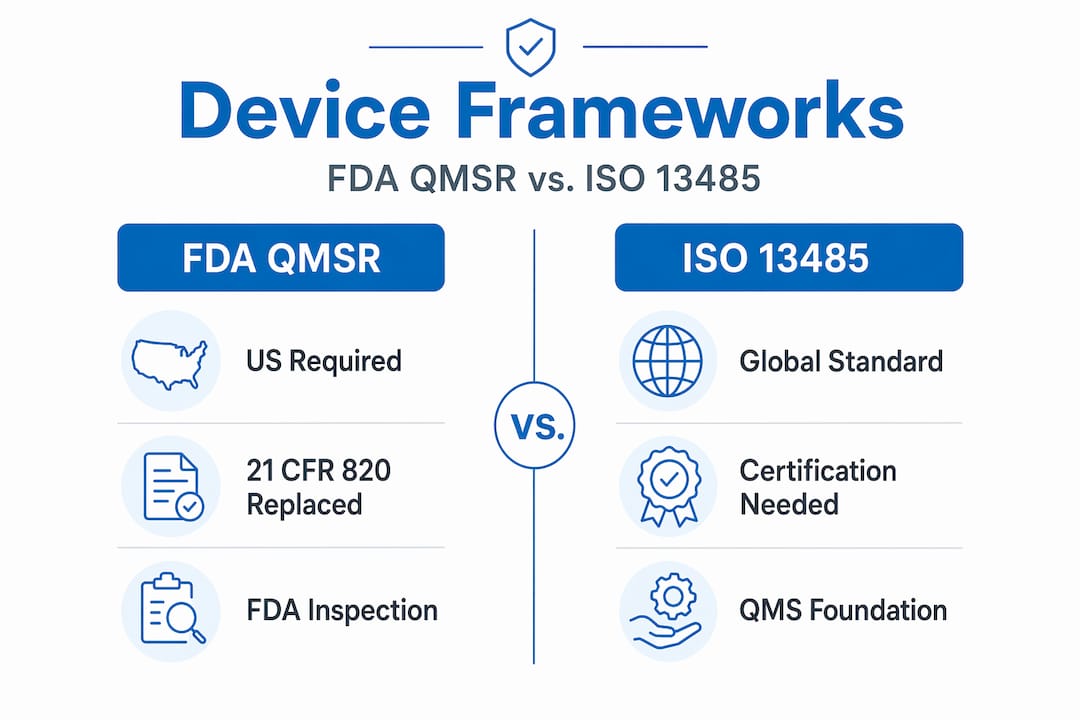
| FDA QMSR is now in effect | As of February 2026, QMSR replaces 21 CFR Part 820 and incorporates ISO 13485:2016 into US requirements. |
| EU MDR backlog remains severe | Over 15,000 MDR applications are still pending, making submission quality a critical factor in certification speed. |
| Regulatory reliance cuts timelines | MDSAP and reliance programs can reduce global registration time by up to 50% when used strategically. |
| ISO 13485 does not exempt FDA inspections | Manufacturers must maintain FDA-specific records including DHF, DMR, and DHR regardless of ISO certification status. |
| Lifecycle compliance is non-negotiable | Risk management, post-market surveillance, and change control must be integrated across every product phase. |
Medical device regulatory frameworks: a global overview
Medical device regulation is not a single system. Across major markets, distinct regulatory authorities apply their own classification logic, conformity assessment pathways, and enforcement mechanisms. Understanding who regulates what, and how devices are categorized, forms the foundation of any compliant market entry strategy.
The three most influential regulatory bodies globally are:
- FDA (United States): Regulates devices under 21 CFR Parts 800-898. Devices are classified as Class I (low risk), Class II (moderate risk), or Class III (high risk), with corresponding submission pathways.
- European Commission and Notified Bodies (EU): Under EU MDR (Regulation 2017/745), devices are classified I through III based on risk, duration, and invasiveness. CE marking is required for market access.
- IMDRF member authorities: Including Health Canada, TGA (Australia), PMDA (Japan), and HSA (Singapore), these regulators increasingly participate in harmonization initiatives to align their national frameworks with internationally recognized standards.
Classification directly governs the approval pathway. A Class II device in the US typically requires 510(k) clearance. 510(k) clearance generally takes 3 to 6 months, while a Class III device requiring Premarket Approval (PMA) can take 2 to 5 years, given the volume of clinical data and post-market obligations involved. CE marking under EU MDR requires Notified Body review for most Class IIa, IIb, and III devices, with timelines discussed in detail below.
ISO 13485 certification is the most recognized global quality management standard and underpins both FDA QMSR compliance and EU MDR conformity assessment. However, manufacturers should treat it as a foundation, not a finish line.
FDA QMSR: what changed in 2026 and why it matters
The shift from the Quality System Regulation (21 CFR Part 820) to the new QMSR is the most significant US regulatory change for device manufacturers in over two decades. QMSR incorporates ISO 13485:2016 by reference, replacing the older prescriptive framework with one centered on risk-based thinking, management responsibility, and demonstrated system effectiveness.
Several specific areas demand attention from compliance teams:
- Management responsibility: Top management must now show documented commitment to quality objectives and system review, not just sign off on procedures.
- Risk-based approach: Design controls, supplier qualification, and corrective actions must all connect to documented risk assessments.
- Supplier oversight: Supplier controls receive heightened scrutiny. Expectations now include risk-tiered supplier qualification, performance monitoring, and documented re-evaluation cycles.
- Internal audits: Audit programs must be risk-based and generate findings that feed into management reviews and CAPA processes.
FDA inspections under QMSR use two models. Model 1 focuses on a specific product or process. Model 2 conducts a full quality system evaluation. FDA inspections now evaluate internal audits and supplier controls more rigorously than under the old QSR framework, meaning documentation gaps that were previously minor findings can now become major observations.
One persistent misconception is worth addressing directly: ISO 13485 certification does not exempt a manufacturer from FDA inspections. Manufacturers must still maintain FDA-specific records including the Design History File (DHF), Device Master Record (DMR), and Device History Record (DHR), which have no direct equivalent in ISO 13485. These records remain FDA requirements under QMSR regardless of certification status.
Pro Tip: Conduct a structured gap assessment mapping your existing ISO 13485 quality management system against QMSR-specific additions before your next scheduled FDA inspection. The gaps are real, and inspectors know where to look.
EU MDR certification challenges and practical strategies
The EU MDR Notified Body capacity crisis is not resolving quickly. The certification process averages 13 to 18 months for technical review, plus a 6 to 12 month intake queue, placing total timelines at approximately 24 months from first contact to certificate issuance. With 33,175 MDR applications submitted, 17,549 certificates issued, and over 15,000 still pending, the backlog affects nearly every device category.

The data tells a clear story for manufacturers planning EU market access:
| Timeline Stage | Duration |
|---|---|
| Intake queue (before review begins) | 6 to 12 months |
| Technical file review | 13 to 18 months |
| Total from first NB contact to certificate | Approximately 24 months |
| Additional delay per query cycle | 6 to 12 weeks |
The most controllable variable in this process is submission quality. Incomplete or poor-quality technical files are responsible for most Notified Body review delays, adding 6 to 12 weeks per query cycle. A single avoidable query can set a program back by a quarter. Conversely, manufacturers who submit thorough technical files move significantly faster through certification.
Clinical evidence requirements under EU MDR are also stricter than legacy MDD standards. Clinical evaluation reports must demonstrate clinical benefit, acceptable risk-benefit profile, and alignment with the state of the art. Post-market clinical follow-up (PMCF) plans are mandatory for most implantable and Class III devices. Post-market surveillance systems must be active and documented, not retrospective.
Proposed revisions to EU MDR and IVDR are in discussion at the European Commission level, primarily targeting transition timelines and legacy device provisions. Until final revisions are published, manufacturers should operate against current requirements without assuming deadline extensions.
Pro Tip: Commission an independent pre-submission technical file audit before engaging your Notified Body. Firms that do this systematically report fewer queries and shorter review cycles. This is not a cost. It’s a timeline hedge.
Global reliance frameworks and multi-market strategy
Regulatory reliance is reshaping how manufacturers approach simultaneous multi-market submissions. At its core, regulatory reliance allows authorities to use assessments completed by other trusted regulators, reducing duplicative work and accelerating market access. This is not theoretical. Reliance programs can reduce global registration timelines by up to 50% and generate material cost savings across a multi-country portfolio.
The IMDRF Playbook provides a structured methodology for regulatory authorities to adopt reliance, and major authorities including FDA, the European Commission, PMDA, HSA, and TGA now actively participate in or recognize reliance outcomes.
The most practical reliance mechanism currently available is the Medical Device Single Audit Program (MDSAP). A single MDSAP audit satisfies quality management system requirements in five countries: the United States, Canada, Australia, Brazil, and Japan. For manufacturers targeting any combination of these markets, MDSAP is almost always the more resource-efficient path.
Key reliance types and their practical implications include:
- Unilateral recognition: One authority accepts the decision of another without conditions. Common in smaller markets referencing FDA or EU decisions.
- Work-sharing: Two or more authorities divide review responsibilities and share findings. Reduces duplicated assessment labor.
- Parallel review: Authorities conduct simultaneous assessment using the same submission package. Requires coordinated submission timing.
- Informed review: An authority uses another’s assessment as a reference but conducts its own evaluation. Provides efficiency gains without full reliance.
For manufacturers entering Southeast Asian markets, HSA Singapore’s regulatory compliance requirements are increasingly aligned with IMDRF frameworks, and ASEAN pilot reliance programs are actively underway. Structuring technical documentation for reuse across these pathways from the outset reduces rework and accelerates multi-market access.
Best practices for lifecycle compliance in 2026
Regulatory compliance does not end at market authorization. The full device lifecycle, from design input through post-market surveillance and product change, requires integrated compliance management. Risk management must connect design control, validation, and post-market surveillance activities into a documented, auditable system.
A lifecycle compliance program that holds up under inspection typically includes the following elements:
- Risk management files updated continuously. Risk assessments are living documents. Any product modification, field complaint trend, or updated clinical data should trigger a risk file review.
- Post-market surveillance systems that generate data. Both FDA and EU MDR require active PMS. Systems relying on complaint logs alone are no longer adequate. Proactive data collection from literature, registries, and field reports is expected.
- Change control documentation that links to regulatory impact assessment. Every product or process change must be evaluated for regulatory significance before implementation. Changes that modify performance specifications, materials, or sterility processes can trigger new conformity assessment obligations under EU MDR.
- Management reviews that actually function as quality inputs. Reviews should aggregate PMS data, audit findings, CAPA trends, and supplier performance into documented management decisions. This is exactly what Notified Bodies and FDA inspectors evaluate for evidence of a functioning quality management system.
- Inspection readiness maintained continuously. Quality manuals, SOPs, and training records should be audit-ready at all times, not refreshed only when an inspection is scheduled.
Adopting a risk-based quality approach is no longer a best practice recommendation. Under both QMSR and EU MDR, it is a regulatory expectation embedded in the conformity assessment criteria.
Pro Tip: Treat your management review as an inspection preparation tool, not a compliance checkbox. Inspectors read management review minutes carefully. If the minutes show that quality data was reviewed and no actions were taken, that absence of action must be explained.
How Labgistics supports your regulatory compliance journey
Medical device manufacturers operating in Southeast Asia face the combined pressure of global regulatory demands and regional market entry requirements. Labgistics brings over 20 years of specialized healthcare logistics experience to help manufacturers manage this complexity with confidence.
Labgistics offers regulatory services for medical devices across Southeast Asia, including submission support, product registration guidance, and compliance consulting aligned with HSA, ASEAN, and international frameworks. For manufacturers requiring controlled storage and distribution, Labgistics operates fully accredited distribution centers with cold chain capability and calibration services critical for maintaining device quality standards. The integrated supply chain solutions Labgistics provides are purpose-built for healthcare logistics risk management, giving device manufacturers a single, accountable partner from registration through distribution.
FAQ
What is FDA QMSR, and when did it take effect?
FDA’s Quality Management System Regulation (QMSR) took effect on February 2, 2026, replacing 21 CFR Part 820 and incorporating ISO 13485:2016 by reference into US quality system requirements.
How long does EU MDR Notified Body certification take?
The process averages approximately 24 months from first contact to certificate issuance, combining a 6 to 12 month intake queue with a 13 to 18 month technical review period.
Does ISO 13485 certification replace FDA inspection requirements?
No. ISO 13485 certification does not exempt manufacturers from FDA inspections. Device History Files, Design History Files, and Device Master Records must be maintained to FDA-specific standards under QMSR regardless of ISO certification status.
What is MDSAP and which countries does it cover?
The Medical Device Single Audit Program (MDSAP) is a single audit that satisfies quality management system requirements in five countries: the United States, Canada, Australia, Brazil, and Japan.
How can regulatory reliance programs benefit multi-market manufacturers?
Regulatory reliance programs allow authorities to use assessments from trusted regulators, reducing duplicate submissions and cutting global registration timelines by up to 50% when applied strategically across target markets.